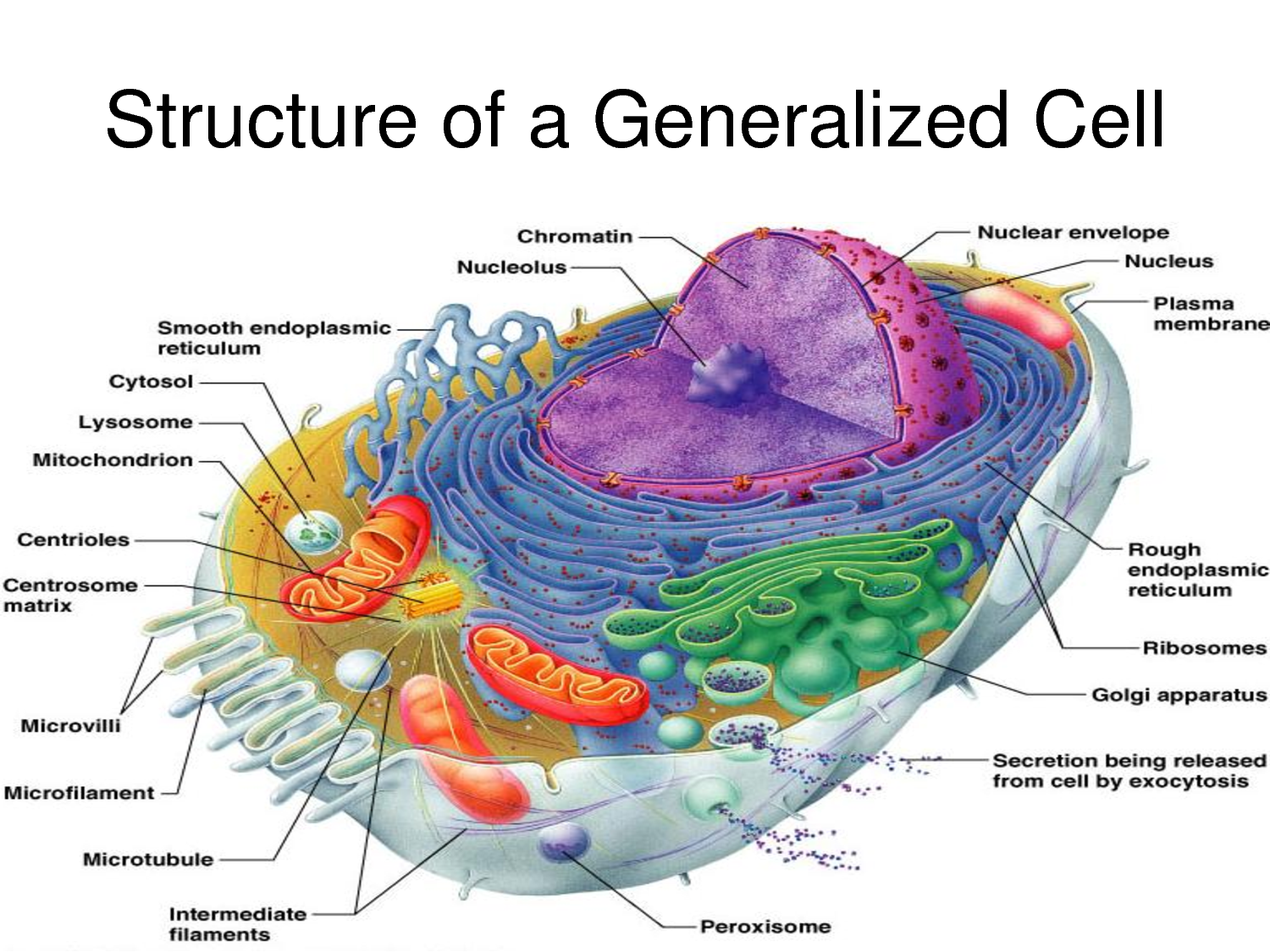
This blog post is a reflection on the modules ‘The Normal Cell’, ‘Cell Injury’ and ‘Cell Death and Necrosis – Gangrene’, from the prescribed text book General Pathology by J.J. Rippey, focussing on the role of the cell in health and disease. Having studied normal cell physiology in the last two years it was good to do a recap of the anatomy of the cell, its organelles and their functions. I will not go into those details here but have included a diagram of a model cell.
 A brief summary of the concepts of the cell theory are that cells are the basic building units of all plants and animals, they are the smallest units that perform all physiological functions vital to life, that all cells come from preexisting cells through the process of division, and that at the cellular level each cell maintains homeostasis. (Martini & Nath, 2009) The role of the cell in health and disease is central as “homeostasis at the level of the tissue, organ, organ system, and organism reflects the combined and coordinated actions of many cells” (Marini & Nath, 2009: 67) and disease can be very broadly defined as an inbalance in homeostasis.
A brief summary of the concepts of the cell theory are that cells are the basic building units of all plants and animals, they are the smallest units that perform all physiological functions vital to life, that all cells come from preexisting cells through the process of division, and that at the cellular level each cell maintains homeostasis. (Martini & Nath, 2009) The role of the cell in health and disease is central as “homeostasis at the level of the tissue, organ, organ system, and organism reflects the combined and coordinated actions of many cells” (Marini & Nath, 2009: 67) and disease can be very broadly defined as an inbalance in homeostasis.
There are many possible aetiologies for cell injury and these include vital substrate deficiency, and physical, chemical or biological insults. (Cobb, et al., 1996) The original injury is a biochemical one and will disrupt or depress, even stop, vital functions of the cell such as energy production by damage to mitochondria, protein synthesis by damage to the endoplasmic reticulum, disruption of the ionic and osmotic steady state by damage to the cell membrane, disruption of reproduction by damage to the nucleus, and generation of reactive oxygen species. (Rippey, 1994) In response to mild and slightly severe injury the cell can adapt so as to restore homeostasis, to protect the cell from further injury (Cobb, et al., 1996) and eventually recover but very severe injury will result in irreversible changes and cell death (Rippey, 1994). Adaptive changes of the cell in response to damage are atrophy, hypertrophy, hyperplasia, and metaplasia. (Badizadegan, 2003) Lets consider hypertrophy. Hypertrophic degeneration of a cell is caused by infiltrations such as water, fat, protein and glycogen. (Rippey, 1994) Cloudy swelling is the accumulation of water in a cell, first as granules and then as vacuoles, and is reversible. Hydropic degeneration is extreme water accumulation, when the vacuoles have coalesced, it may be reversible but usually leads to cell rupture and death. (Rippey, 1994) Fatty change is the accumulation of fat within a cell, first as liposomes close to the endoplasmic reticulum and then as fat vacuoles, it is a more severe form of cell damage even though in its earlier stages it is still reversible. (Rippey, 1994) Hyaline droplets, Russell bodies and Mallory’s hyaline are examples of protein accumulation within a cell. They have an homogenous glassy eosinophilic appearance and indicate very severe injury to a cell and a precursor to cell death. (Rippey, 1994) Glycogen infiltration does not lead to cell death nor functional damage, however it does lead to vacuoles in the cytoplasm and nucleus when there is an excessive accumulation. (Rippey, 1994)
“Cell death is valuable for the organism because it removes terminally injured or unwanted cells that utilise valuable substrates and nutrients.” (Cobb, et al., 1996: 3) Necrosis is the morphological changes – such as cytoplasmic swelling, swelling of the endoplasmic reticulum and mitochondria, blebbing of the plasma membrane, dissolution of chromatin, and loss of membrane integrity (Cobb, et al., 1996) – which occur after cell death in a living body. (Rippey, 1994) Apoptosis is programmed cell death and is manifested by cytoplasmic shrinkage, nuclear chromatin shrinkage and eventually larger plasma membrane buds. (Cobb, et al., 1996) The debris resulting from both types of cell death are engulfed by phagocytic cells. Necrotic debris acts as an irritant to the adjacent living tissue which triggers inflammation, this is called the vital response. Apoptosis does not trigger inflammation. (Rippey, 1994)
There are different types of necrosis. Coagulative necrosis is when the cell becomes an eosinophilic opaque mass with loss of the nucleus, this usually occurs in an infarct of the kidney, prostate, heart, spleen and lung. (Rippey, 1994) Colliquative necrosis is complete destruction of a cell due to total enzymatic dissolution, this usually occurs in a brain infarct. (Rippey, 1994) Suppurative necrosis is a form of colliquative necrosis due to bacterial infection, causing pus formation. Casseous necrosis is associated with tuberculosis, it is when there is a total loss of cell detail due to the cell becoming a mass of amorphous fat and protein. Gummatous necrosis is similar to casseous necrosis but is associated with syphilis. (Rippey, 1994) Fat necrosis is either the enzymatic breakdown of true fat in tissues surrounding the pancreas (enzymatic fat necrosis) or the release of neutral fat from a cell causing inflammation and eventually scarring (traumatic fat necrosis). (Rippey, 1994) Gangrenous necrosis is necrotic tissue that has been invaded by saprophytic putrefactive organisms from the gut or soil, it can only occur in living tissue and, due the presence of oedema in gangrenous tissue, is called moist gangrene. (Rippey, 1994)
 My concept of disease changed after studying the modules above in that I didn’t realise how much our bodies are able to withstand before consciously experiencing disease, how much injury a cell can withstand before it becomes irreversible and leads to cell death. The adaptation that occurs at the deepest levels of the body is astounding, the continual striving for homeostasis by each cell despite damage, resulting in either recovery or cell death and the vital reaction. Also, that the cell’s reaction to injury may contribute to the disease process itself, it seems paradoxical yet by understanding the mechanisms of cellular response to injury it makes sense too.
My concept of disease changed after studying the modules above in that I didn’t realise how much our bodies are able to withstand before consciously experiencing disease, how much injury a cell can withstand before it becomes irreversible and leads to cell death. The adaptation that occurs at the deepest levels of the body is astounding, the continual striving for homeostasis by each cell despite damage, resulting in either recovery or cell death and the vital reaction. Also, that the cell’s reaction to injury may contribute to the disease process itself, it seems paradoxical yet by understanding the mechanisms of cellular response to injury it makes sense too.
References
Badizadegan, K., 2003. Cell injury, adaptation and death, HST.035 Principle and Practice of Human Pathology. Harvard-MIT Division of Health Sciences and Technology, unpublished.
Cobb, J.P., Hotchkiss, R.F., Karl, I.E. and Buchman, T.G., 1996. Mechanisms of cell injury and death. British Journal of Anaesthesia, 77: 3-10.
Martini, F.H. and Nath, J.L., 2009. Fundamentals of Anatomy and Physiology. 8th ed. San Francisco: Pearson Benjamin Cummings.
Rippey, J.J., 1994. General Pathology. Johannesburg: Witwatersrand University Press.

This was a very good contribution. Easy to read, and contained a fair amount of your own insight into these concepts. The middle portions however are to much of a summary, without looking into the assignment core bief (i.e. how you see the cell as a central player in health and disease, and using the ‘facts’ to illustrate your insight and opinion). You videos are great, and embedded into the blog, which is excellent (maybe you can write a short point-by-point instruction for the class on how you do this on wordpress?). However, try refer to images and video selected in your writing. These should have more meaning and not appear to random.